

Why ADL Performance Breaks Down Even When Strength Looks Functional in Occupational Therapy
Understanding How Movement Coordination Influences Activities of Daily Living
Occupational therapists frequently encounter a puzzling situation during rehabilitation. A patient may demonstrate adequate strength during testing, maintain stable sitting balance during evaluation, and clearly understand the task being asked of them. From an impairment perspective, the building blocks for independence appear to be in place. Yet when the patient begins a self-care activity, the task unfolds very differently.
Dressing may take far longer than expected. Grooming may require the patient to brace the opposite arm against the counter for stability. Transfers may look effortful even though lower extremity strength appeared functional during testing.
Many occupational therapists have experienced this exact scenario and wondered why ADL performance still looks unstable or inefficient. The explanation often lies in something that isolated strength testing does not fully capture. Activities of daily living depend not only on strength, but also on how the body organizes movement during real tasks. Observing how movement unfolds during ADL performance is therefore one of the most valuable clinical skills in occupational therapy.
The Common Clinical Scenario in Adult Rehabilitation
Consider a patient who demonstrates fair to good upper extremity strength during evaluation. During testing, the patient is able to lift the arms against resistance, maintain seated posture without external support, and follow directions without difficulty. From a testing perspective, the physical capacity to perform many self-care tasks appears to be present. However, when the patient begins practicing upper body dressing, the movement often looks very different.
As the patient attempts to thread an arm into a sleeve, the trunk may lean slightly to one side. The opposite arm presses into the mattress or chair to help stabilize the body. Movements slow down as the patient works to maintain balance while coordinating the task. Eventually the shirt is on, but the process required far more effort than expected.
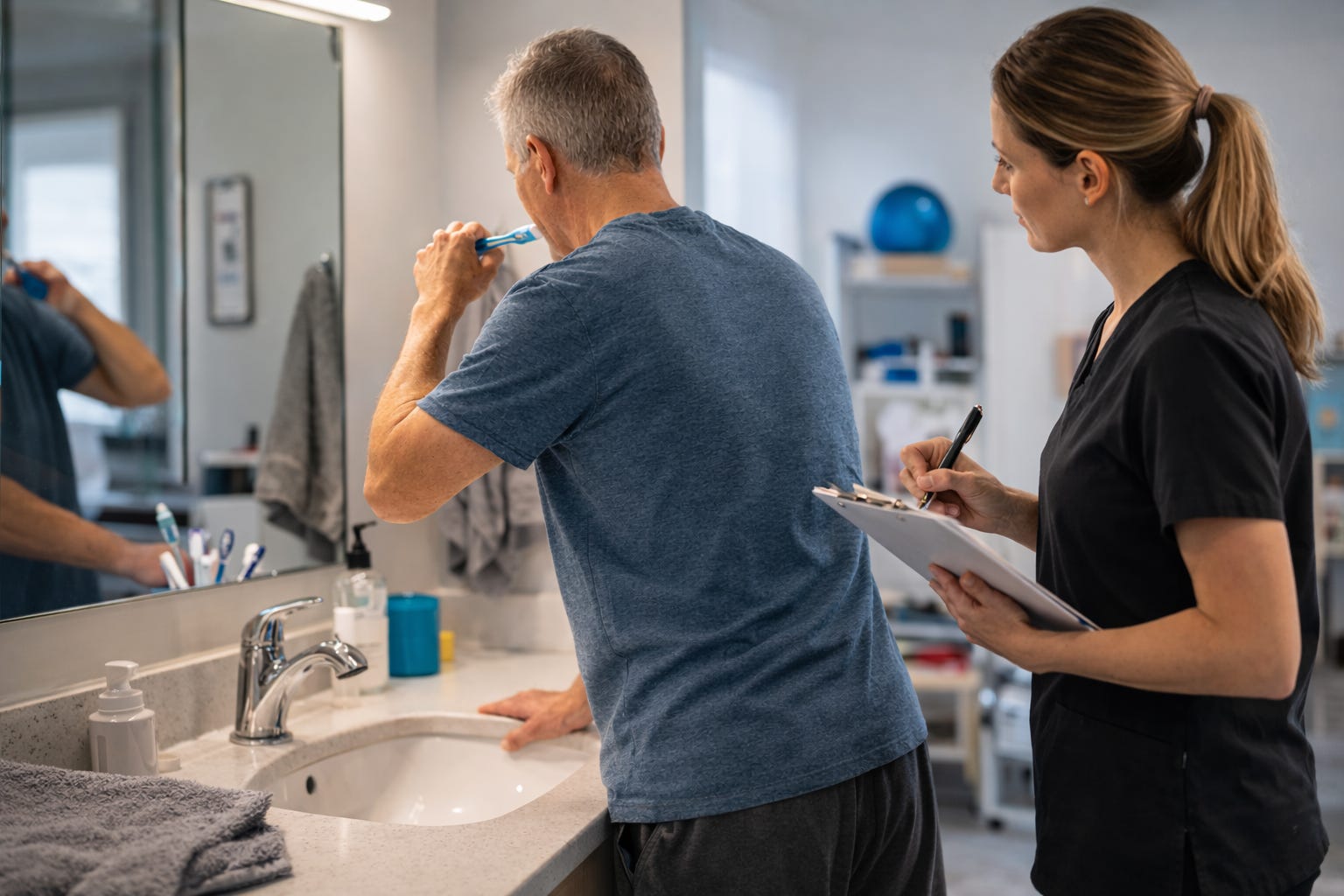
A similar pattern may appear during grooming tasks. The patient may have adequate grip strength to hold a toothbrush or hairbrush, yet when the arm moves away from the body, the trunk begins to sway. To maintain stability, the patient braces against the sink or counter before completing the movement.
Transfers can reveal the same challenge. Lower extremity strength may appear strong during testing, and the patient may push effectively against resistance during manual muscle testing. Yet when standing from a chair, the movement can appear disorganized. The patient may rock forward several times before lift-off, or the movement may look slow and effortful as the body works to coordinate the transition.
For occupational therapists, situations like these highlight an important reality in rehabilitation. Strength alone does not determine how smoothly a functional task unfolds.
Why Strength Does Not Always Translate to ADL Performance
Strength testing provides valuable information during occupational therapy evaluation. It helps clinicians identify clear impairments and guide early intervention planning. At the same time, most ADLs require more than isolated muscle activation. Activities such as dressing, grooming, bathing, and toileting rely on several additional movement components working together.
Functional self-care tasks depend on:
coordinated movement patterns
postural control during limb movement
weight shifting while maintaining balance
timing and sequencing between body segments
These elements allow the body to remain stable while producing movement. When they are working well, ADL performance looks smooth and efficient. Movements flow naturally from one phase of the task to the next. When they become disorganized, the task often begins to break down even when strength appears adequate.
A patient may have enough strength to lift the arm but lose trunk alignment when the arm moves away from the body. Another patient may have strong legs but struggle to coordinate the forward weight shift required for standing. In these situations, the difficulty lies less in muscle force and more in how the body organizes movement during functional activity.
ADLs Require Coordinated Movement Across the Whole Body
Activities of daily living often appear simple because most people perform them automatically. Beneath that automatic behavior, however, these routines rely on coordinated movement across multiple parts of the body.
Dressing provides a clear example. When reaching to pull a shirt over the head, the trunk must maintain alignment against gravity while the arms move overhead. At the same time, the pelvis subtly shifts to allow the shoulders and arms to rotate through space. These adjustments allow the upper body to move freely while the rest of the body remains balanced on the surface below.
When this coordination is working well, the task appears smooth and controlled. When the body struggles to organize these movements, the activity often slows down or requires additional stabilization.
Grooming tasks involve similar demands. Reaching to brush the hair or wash the face requires the trunk to provide a stable base while the arm moves away from the body. Small adjustments occur continuously through the spine and pelvis to keep the body balanced throughout the movement.
Toileting routines often involve even more complex movement sequences. The individual may need to rotate, lean forward, adjust clothing, and return upright while maintaining balance during each phase of the activity.
Across these self-care tasks, the body is constantly managing several movement demands at the same time. Alignment must be maintained against gravity, weight must shift to allow the limbs to move, and multiple body segments must coordinate through a sequence of actions.
When these elements work together effectively, ADL performance tends to look smooth and efficient. When coordination becomes disrupted, the task often becomes slower, less stable, or more effortful.
How Occupational Therapists Analyze Movement During ADLs
One of the most valuable observational skills in occupational therapy is learning to analyze how movement unfolds during everyday tasks. Instead of focusing only on whether the patient completed the task, occupational therapists watch how the body organizes itself during performance.
Several movement patterns can signal that coordination is influencing how an activity of daily living unfolds. These patterns often appear subtly during self-care routines, and once therapists begin watching for them, they become easier to recognize across many tasks.
One common observation occurs when a patient stabilizes the body with the opposite arm during reaching tasks. During grooming, for example, a patient may press the non-dominant arm firmly into the sink or counter while brushing their teeth or combing their hair. During dressing, the patient may place one hand on the bed or chair while the other arm threads into a sleeve. In these situations, the body is often creating a temporary point of stability so the reaching arm can move more safely.
At other times, the trunk itself moves excessively as the arms reach. When a patient reaches for clothing during dressing or reaches toward grooming supplies on a counter, the trunk may sway or lean noticeably with the arm movement. Instead of the trunk providing a steady base, the entire upper body moves together with the reaching arm. As a result, the movement often becomes slower and more cautious as the patient works to maintain balance.
Pauses during movement can provide another clue. A patient performing lower body dressing may begin reaching toward the feet, pause briefly to regain balance, and then continue the movement in smaller segments. Similar pauses may appear during grooming routines when the patient stops between brushing strokes or between steps in the task. These moments often reflect the body reorganizing posture before continuing the activity.
Movement transitions during ADLs may also lose their fluidity. When dressing at the edge of the bed, for instance, a patient may lean forward to reach toward clothing, return upright to regain stability, and then lean forward again to complete the task. Instead of flowing through the movement sequence, the body repeatedly resets its position before continuing.
Environmental supports frequently become part of these strategies as well. A patient may keep one forearm resting on the counter throughout grooming, grip armrests firmly during transfers, or brace against the mattress while dressing at the bedside. These supports often allow the task to be completed successfully, but they also reveal how the body is working to maintain stability during movement.
For occupational therapists, observing these behaviors provides valuable insight into how movement coordination is shaping ADL performance. Rather than focusing only on whether the task was completed, watching how the body organizes itself during the activity helps identify where movement is becoming less efficient and where intervention may be most helpful.
Once occupational therapists begin paying attention to these movement behaviors, it becomes easier to recognize how the body is organizing itself during everyday tasks. These observations often reveal where stability is being created, where movement becomes less controlled, and where the body is compensating to complete the activity. Watching these small details helps clarify why a task feels inefficient or unstable even when basic strength and range of motion appear functional.
Connecting Movement Analysis to Occupational Therapy Intervention
When occupational therapists begin recognizing these movement patterns during ADL performance, treatment planning often becomes much more precise. Instead of focusing primarily on general strengthening, intervention can target the specific movement demands that are interfering with the task itself.
Many difficulties during activities of daily living occur because the body is struggling to organize movement while maintaining stability. By analyzing how the trunk, pelvis, and limbs are working together during the activity, occupational therapists can identify exactly where movement is becoming less efficient.
For example, bathing routines often require the body to maintain balance while the arms move in multiple directions. When reaching to wash the lower legs or feet, the trunk must remain aligned while the body leans forward and the arms extend downward. If trunk control is limited, the patient may hesitate before reaching, pause midway through the movement, or rely heavily on the shower wall or grab bars for stability.
Lower body dressing can reveal similar coordination demands. When stepping into pants or lifting one foot to put on socks, the body must shift weight onto one leg while the other leg moves freely. If weight shifting is poorly organized, the patient may repeatedly reset their posture, grab onto nearby furniture, or avoid lifting the foot very far from the floor.
Meal preparation tasks can also highlight movement coordination challenges. Reaching into cabinets, carrying items across the kitchen, or placing dishes into a dishwasher requires the trunk to stabilize while the arms move away from the body. When coordination is limited, the patient may move the entire body toward the object instead of reaching, take extra steps to stay balanced, or pause frequently while repositioning.
Even simple activities like putting on shoes can reveal movement organization challenges. Leaning forward to reach the feet requires the trunk to control forward movement while the arms guide the shoe into place. If that coordination is disrupted, the patient may struggle to maintain balance, repeatedly adjust their posture, or rely on the bed or chair for additional support.
Understanding these movement demands allows occupational therapists to design treatment activities that directly address the underlying challenge while still supporting functional independence.
Intervention may include practicing reaching movements while maintaining trunk alignment. A therapist might guide the patient through controlled reaching activities while seated at the edge of the bed or standing at a counter, encouraging the trunk to remain stable as the arm moves through space.
Structured weight shifting activities may also be used to help the patient free one limb for movement while maintaining balance. For example, practicing small lateral or forward weight shifts can prepare the body for tasks such as stepping into pants, reaching toward the feet during dressing, or adjusting clothing during toileting.
Therapists may also work on improving movement transitions between positions. Practicing controlled forward weight shifts, partial sit-to-stand movements, or repeated sit-to-stand transitions can help the body coordinate the timing between trunk movement and lower extremity activation.
As these movement patterns become more organized, ADL performance often becomes noticeably smoother. The patient may rely less on bracing during grooming tasks. Dressing routines may occur with fewer pauses as balance improves during reaching. Transfers may begin to look more fluid as the body coordinates weight shifting and trunk movement more effectively.
In many cases, functional improvement occurs not simply because the patient became stronger, but because the body learned to coordinate movement more efficiently during the task itself.
A Shift in How Occupational Therapists Observe Function
When occupational therapists begin analyzing movement during activities of daily living, the way they observe functional tasks often changes. Rather than focusing only on whether the patient completes the task, attention shifts toward how the movement unfolds throughout the activity.
This perspective encourages therapists to look beyond isolated impairments and consider how different parts of the body work together during everyday routines. Small adjustments in posture, timing, and balance often reveal important information about how the body is managing the task.
For many clinicians, this shift strengthens clinical reasoning. Instead of documenting that an activity is difficult or inefficient, therapists can begin identifying the specific movement demands influencing performance.
Over time, self-care activities start to look less like a series of simple steps and more like coordinated movement sequences. Observing how the body organizes these sequences helps occupational therapists better understand why tasks become unstable, effortful, or slow, and where intervention may be most effective.
Watching Movement Inside Everyday Tasks
One of the most powerful habits occupational therapists can develop is closely observing how movement unfolds during everyday activities. During dressing, notice how the patient shifts weight when the arms move. During grooming, watch how the trunk responds when the arm reaches away from the body. During transfers, observe the timing between trunk movement and lower extremity activation. These small details often reveal the true challenges influencing ADL performance.
Strength will always remain an important component of rehabilitation. At the same time, analyzing movement during activities of daily living allows occupational therapists to identify the factors that determine whether a task feels smooth, stable, and efficient. For many clinicians, this shift in perspective becomes a turning point in clinical reasoning. Instead of asking only whether the patient has enough strength for the task, the question becomes:
How is the body organizing movement during the task itself?
Once occupational therapists begin looking at ADL performance through that lens, everyday activities reveal an entirely new level of clinical insight.
If you enjoy analyzing the movement patterns behind everyday activities, OT Practice Toolkit explores these ideas every week. The free newsletter shares clinical insights on ADL performance in adult rehabilitation. Paid subscribers receive deeper guidance on intervention strategies and documentation approaches that translate movement analysis into clear clinical reasoning.